URGENT!
Congress and the Trump Administration are considering drastic cuts to the Medicaid program that could affect more than 1.4 million Minnesotans and the financial viability of medical practices and hospitals across the state. Physicians need to fight back now to protect patients’ access to Medicaid. Here’s how.
Calls to Action
Background
Congress and Medicaid Cuts
On February 25, the U.S. House of Representatives adopted a budget resolution (i.e., budget plan) that includes a $880 billion target for cuts to programs under the jurisdiction of the House Energy and Commerce Committee. This includes Medicare, Medicaid, and the Children’s Health Insurance Program (CHIP). It is now up to the Committee to propose how those cuts should be made.
While much is uncertain, two things are clear. First, President Trump has consistently said he will not sign a budget that includes cuts to Medicare. Second, if Medicare cuts are off the table, the Congressional Budget Office (CBO) has indicated that the House Energy and Commerce Committee cannot make $880 billion in cuts without cuts to Medicaid.
Meanwhile, the U.S. Senate has adopted its own budget resolution that directs Senate committees, including committees with oversight over Medicaid, to identify at least $4 billion in spending cuts. Although the current Senate target is lower, the two chambers need to agree on a final target for which Medicaid remains at particular risk.
Timeline
The time to act is now!
House and Senate leadership are working to reconcile their budget targets by mid-April. House leadership has indicated its goal to get a final budget signed by the president by the end of May.
Medicaid in Minnesota
Medicaid is a joint federal-state program that provides health insurance and long-term care coverage to low-income individuals. Minnesota’s version of Medicaid is called Medical Assistance (MA).
To be eligible for MA, individuals must meet income requirements that vary by age, pregnancy status, and family size. People enrolled in MA pay no premium for coverage and no cost sharing for a comprehensive list of health services.
In 2023, roughly one-in-four Minnesotans were enrolled in MA (i.e., 24.4%). MA covers 41% of Minnesota children and 30% of births in the state. Its impact is even greater in Black and Indigenous communities – MA covers 80% of births of Black babies and 90% of births of Indigenous babies in Minnesota.
MA plays a pivotal role in minimizing Minnesota’s uninsured rate, which sits at an all-time low of 3.8%. Minnesotans covered by public programs, like MA, are half as likely to delay or forgo care due to cost compared to uninsured Minnesotans (i.e., 26% and 53%, respectively).
Moreover, Minnesota spends more than 60% of MA funds on services and support for the elderly and people with disabilities. MA, not Medicare, is the primary source of coverage for people who need long-term care services, like nursing homes, in Minnesota.
Vulnerable Minnesotans in every corner of the state depend on MA. While counties in metropolitan areas have relatively high counts of MA enrollees, counties in greater Minnesota have relatively high percentages of their populations enrolled in MA.
However, because MA is a joint federal-state program, its future impact is limited by federal funding and guidelines.
Congressional Options
There are various ways in which Congress might pursue cuts to Medicaid, including, but not limited to, the list below. All these mechanisms serve to shift costs to states and reduce coverage for low-income individuals (i.e., through decreases in eligibility, decreases in covered services, and/or increases in premiums and cost-sharing).
- Reduce Federal Matching Rates. Right now, for every dollar the Minnesota government spends on Medicaid for children and parents, the federal government contributes 51.2 cents. For every dollar the Minnesota government spends on Medicaid for childless adults, the federal government contributes 90 cents. Congress could decide to drastically reduce one or both match rates. Reduced federal match rates would shift costs to Minnesota, and Minnesota would be forced to (a) reduce MA coverage, (b) reduce physician and other provider payments, (c) raise taxes, and/or (d) cut funding for other important state priorities (e.g., schools, roads, public safety).
- Impose Caps on Federal Matching Funds. Right now, there is no cap on how much states can receive in federal matching funds under Medicaid. Congress could impose per-capita or absolute (i.e., aggregate) caps on federal matching funds. Caps would shift costs to Minnesota, and Minnesota would be forced to (a) reduce MA coverage, (b) reduce physician and other provider payments, (c) raise taxes, and/or (d) cut funding for other important state priorities (e.g., schools, roads, public safety).
- Switch to State Block Grants. Right now, the amount the federal government gives to any one state for Medicaid is a set percentage of that state’s spending level for Medicaid (i.e., through a federal matching rate system). This system ensures that states receive additional funds in proportion to any increases in enrollment and/or healthcare costs. Congress could instead switch to a block grant system, wherein states are given a lump sum of federal dollars at the outset of each year. Block grants would shift to states the full cost of unexpected increases in MA enrollment (e.g., during economic downturns) and/or MA healthcare costs (e.g., during disease outbreaks or older/sicker enrollees).
- Impose Work Requirements. Right now, there is no national requirement that working-age Medicaid recipients actively seek or obtain employment. Congress could require that working-age Medicaid recipients regularly file paperwork to prove that they work for a minimum of x hours per week, where x is determined by Congress. According to a 2023 KFF survey, an estimated 92% of working-age Medicaid recipients were already working full- or part-time or were not working because they were a caregiver, had an illness or disability, or were in school. The Congressional Budget Office, a nonpartisan research office, has concluded that, if work requirements were implemented, “about 1.5 million adults…would lose…Medicaid coverage” and “the employment status of and hours worked by Medicaid recipients would be unchanged.”
The True Costs of Medicaid Cuts
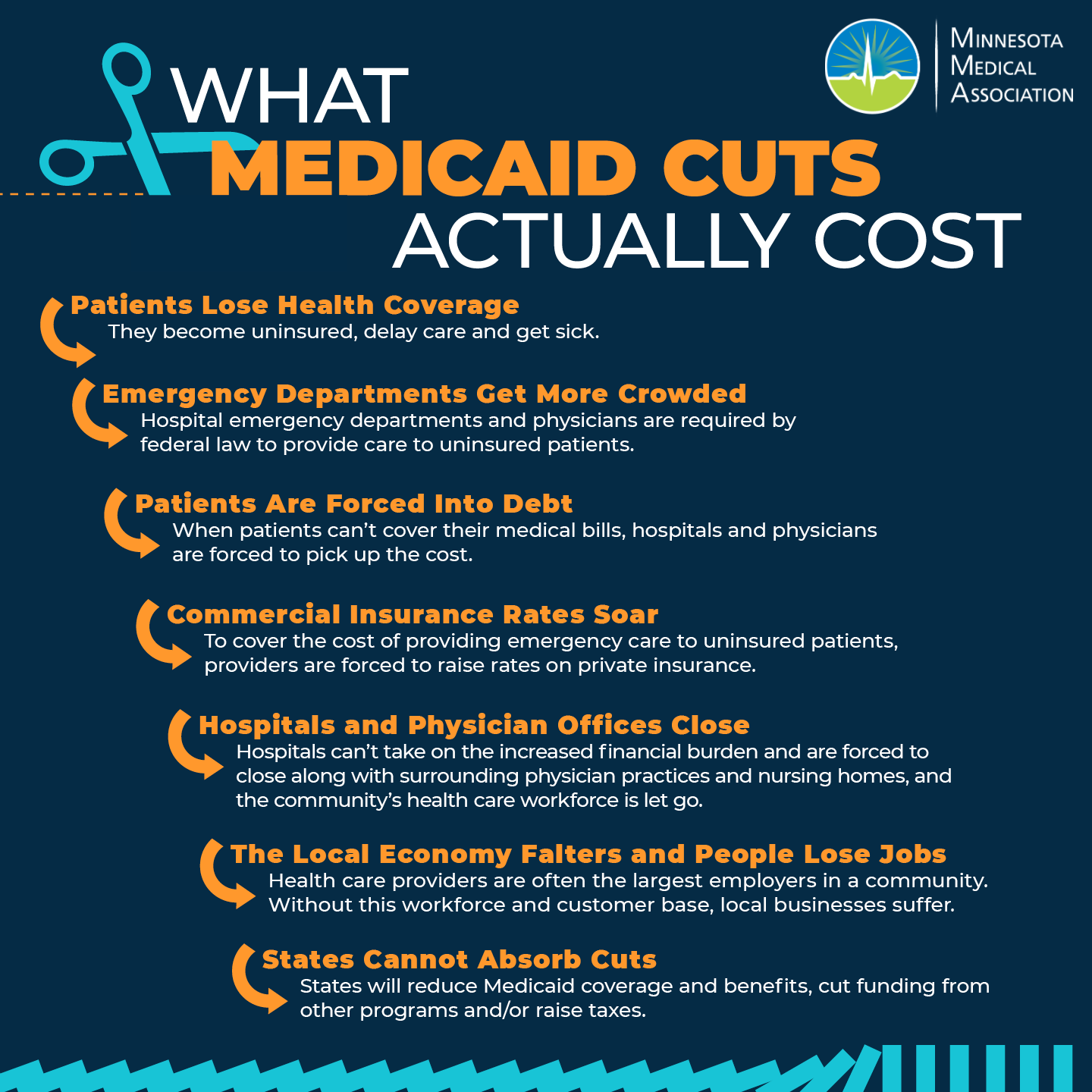
You are welcome to share this image. Please right-click to copy or save to your computer.
Other Resources
- “Medicaid Matters Communications Toolkit,” Minnesota Department of Human Services
- “Medicaid: Protecting Health Care for Minnesotans,” Minnesota Hospital Association
- "Social Media Toolkit," Physicians for Medicaid
- "Take Action," Physicians for Medicaid